Hi, I'm Brendan. Thanks for stopping by to read about me and my life with a rare blood disorder called Aplastic Anemia.
Unlike most blogs, this one reads chronologically - from the top down. This means that you will have to scroll all the way to the bottom of the page to find the most recent post. I am keeping it this way so that my story is not read in reverse order.
If the site color scheme is a little too dark for you, click here to view a pdf that is black text on a white background.
Please also make sure to check out the "other AA stories" section on my sidebar and visit those sites as well. Mine is only one of many Aplastic Anemia survivor stories, and they're all worth checking out.
7.21.2005
I went swimming on this night. As usual, I started each set strong and hit a wall almost immediately, with my arms and legs becoming jello-esque after only a few laps. The carbs I loaded up on before hand, and the Gatorade I drank during breaks might as well have been chili cheese fries and a root beer float. At the end of practice, the coach surprised us with a couple of relay races instead of the normal boring cool-down. Considering how poorly I fared during most of our longer sets, he paired me with a swimmer that was in much better shape to “even things out.” We won the relay, but I was absolutely exhausted afterwards. All-out sprinting at the end of the workout was probably not a good thing for me to do. I had to lay down on the deck for a few minutes before I could walk into the locker room. After getting changed I rested some more because I knew I would need it for the walk to my car. I don’t think I had ever felt so tired. Sitting in my car, I didn’t immediately drive off because I wasn’t completely sure that I wasn’t going to pass out. It was a full hour and a half before I felt okay again, and my body no longer felt like it was going to shut down.
I had been swimming most every Thursday since the beginning of June – as that night was the one I had signed up to swim with the Master’s team at the YMCA. Back when I started, I thought that I would gradually get into better shape and maybe even pick up another day or two a week. I had heard about a different group’s Sunday morning practice, and even emailed the coach of that group to let him know that he should expect me to start working out with them within a few weeks. That never happened. In fact, the Thursday night practices seemed to get harder, not easier. During one July week, my coach asked me if I was getting any other exercise besides the swimming. He said it with such disdain that I was too embarrassed to let on that I had in fact been eating healthier, taking walks at night, and riding my exercise bike several times a week. Instead I played dumb while he explained to me that I should really try to exercise more, even if just to take a few walks or use the stairs instead of the elevator.
I had been swimming most every Thursday since the beginning of June – as that night was the one I had signed up to swim with the Master’s team at the YMCA. Back when I started, I thought that I would gradually get into better shape and maybe even pick up another day or two a week. I had heard about a different group’s Sunday morning practice, and even emailed the coach of that group to let him know that he should expect me to start working out with them within a few weeks. That never happened. In fact, the Thursday night practices seemed to get harder, not easier. During one July week, my coach asked me if I was getting any other exercise besides the swimming. He said it with such disdain that I was too embarrassed to let on that I had in fact been eating healthier, taking walks at night, and riding my exercise bike several times a week. Instead I played dumb while he explained to me that I should really try to exercise more, even if just to take a few walks or use the stairs instead of the elevator.
8.14.2005
On July 25th, 2005 I called my internist to see if they could squeeze me in that day. It was a Monday, and the day before I had experienced some odd blurred vision and a headache, along with just generally feeling out of shape for the last month or so. They told me that they couldn’t move up the general checkup appointment I had for the following week – but they could fit me in at 2:15 pm just to see about what had happened over the weekend. It was actually the first time I had ever met this doctor, so he had little to go off of as far as my medical history went. Despite that, he was concerned enough with my pale appearance (including almost white lips) and random leg bruises (that I couldn’t recall getting) to order a set of blood tests. I didn’t think much of it at the time, mostly expecting this to result in him telling me to get more sleep or eat more vegetables.
He called me that night with the test results, at around 7:30 pm. I was on my way to the grocery store to do some shopping. He told me that my blood levels (white blood cell, red blood cell, and platelet) were critically low, and that I would need to be admitted into the hospital that night for further testing. A little worried at this point, I followed his orders and had my girlfriend drive me to St. John’s Mercy Medical Center. The night doctor ran through the gamut of what could be causing my abnormally low blood counts – stressing that we needed further testing before coming to any conclusions. Very early the next morning, at about 6 or 7 am, I was awakened by a new doctor – an oncologist/hematologist named Dr. Mary Klix. She introduced herself, and then jumped right into a conversation about Leukemia treatments. That scared me. I stopped her and asked her if she was telling me I had Leukemia? Like the previous doctor she wouldn't say for sure, but she was about 90% sure. Further tests, including a bone marrow biopsy, were necessary, she said.
The bone marrow biopsy was done on Wednesday morning. It's technically called an “aspiration” which is just a fancy way of saying that they jammed a mean looking syringe into my hip and sucked out a marrow sample. I wouldn't say that the procedure hurt, but it definitely felt weird. It's not often that you feel pressure from inside your iliac crest.
Thursday afternoon the results came back. I did not have Leukemia. I had Aplastic Anemia. As I write this, that diagnosis was 17 days ago. I spent 10 days in the hospital, 4 of which were devoted to my chemotherapy – ATG (Antithymocyte Globulin). Now I’m back at my apartment, continuing drug therapy (Methylprednisolone and Cyclosporine) and returning to the hospital’s cancer center several times a week for blood tests and transfusions as needed. How much more do I have to go? Weeks? Months? Years? Will this treatment need to be repeated? What about transplant? These are only a few of the questions I don’t have answers for. I hope that with time I will find the answers to some of these questions, and learn to not worry so much about the ones I can't answer.
UPDATE 3/17/2010: I now have a copy of my medical records. These are results from my first CBC & Platelets upon admittance to SJMMC. Click image to enlarge it.

He called me that night with the test results, at around 7:30 pm. I was on my way to the grocery store to do some shopping. He told me that my blood levels (white blood cell, red blood cell, and platelet) were critically low, and that I would need to be admitted into the hospital that night for further testing. A little worried at this point, I followed his orders and had my girlfriend drive me to St. John’s Mercy Medical Center. The night doctor ran through the gamut of what could be causing my abnormally low blood counts – stressing that we needed further testing before coming to any conclusions. Very early the next morning, at about 6 or 7 am, I was awakened by a new doctor – an oncologist/hematologist named Dr. Mary Klix. She introduced herself, and then jumped right into a conversation about Leukemia treatments. That scared me. I stopped her and asked her if she was telling me I had Leukemia? Like the previous doctor she wouldn't say for sure, but she was about 90% sure. Further tests, including a bone marrow biopsy, were necessary, she said.
The bone marrow biopsy was done on Wednesday morning. It's technically called an “aspiration” which is just a fancy way of saying that they jammed a mean looking syringe into my hip and sucked out a marrow sample. I wouldn't say that the procedure hurt, but it definitely felt weird. It's not often that you feel pressure from inside your iliac crest.
Thursday afternoon the results came back. I did not have Leukemia. I had Aplastic Anemia. As I write this, that diagnosis was 17 days ago. I spent 10 days in the hospital, 4 of which were devoted to my chemotherapy – ATG (Antithymocyte Globulin). Now I’m back at my apartment, continuing drug therapy (Methylprednisolone and Cyclosporine) and returning to the hospital’s cancer center several times a week for blood tests and transfusions as needed. How much more do I have to go? Weeks? Months? Years? Will this treatment need to be repeated? What about transplant? These are only a few of the questions I don’t have answers for. I hope that with time I will find the answers to some of these questions, and learn to not worry so much about the ones I can't answer.
UPDATE 3/17/2010: I now have a copy of my medical records. These are results from my first CBC & Platelets upon admittance to SJMMC. Click image to enlarge it.

8.26.2005
I stopped taking my Methylprednisolone steroid today.
Full dosage actually stopped on 8/18 (for a total of two weeks at full dose, starting when released from the hospital on 8/4). Tapering began on 8/19, by decreasing the dosage every two days – ending up with the last one today.
Before I started taking it, my doctor told me that possible side effects could be weakness in the thighs, increased appetite, and fat face (bloating). I experienced only minimal thigh weakness, and a ridiculous appetite that resulted in me consuming what was probably two or three times the healthy amount of food for one individual. As far as fat face goes, I’m pretty sure I didn’t experience anything close to that – besides maybe fat waistline from the crazy amount of food I inhaled. In any case, I took head shots of myself with my camera phone to chronicle any possible fat face-ness. Check those pictures out here.
Full dosage actually stopped on 8/18 (for a total of two weeks at full dose, starting when released from the hospital on 8/4). Tapering began on 8/19, by decreasing the dosage every two days – ending up with the last one today.
Before I started taking it, my doctor told me that possible side effects could be weakness in the thighs, increased appetite, and fat face (bloating). I experienced only minimal thigh weakness, and a ridiculous appetite that resulted in me consuming what was probably two or three times the healthy amount of food for one individual. As far as fat face goes, I’m pretty sure I didn’t experience anything close to that – besides maybe fat waistline from the crazy amount of food I inhaled. In any case, I took head shots of myself with my camera phone to chronicle any possible fat face-ness. Check those pictures out here.
9.15.2005
It’s been a month and a half since I went into the hospital.
I have stopped taking the Zyrtec, which was prescribed to abate possible reactions to the steroid and other medications. I’m also attempting to stop taking the Prilosec, which was for stomach/GI discomfort due to the Cyclosporine.
I am still taking the Cyclosporine, twice a day at a dosage level only recently pinpointed - after several trials at both higher and lower dosages. There is a specific level that my doctor would like to see in my blood – and for a few weeks we seemed to not be able to hit that target. I would take one dose and end up with nearly toxic levels in my blood, so then we’d drop that dose down and end up with levels that barely registered. Anyway, we eventually got it right – and I’m attempting to do it without the accompanying Prilosec (but not without the accompanying Nystatin). So far so good.
One thing I’ve learned about this whole process that I wasn’t prepared for is that it isn’t one furious sprinting battle that I’m fighting, but several much smaller long-term ones. And for me, that is harder. I’d rather attack like crazy and get it over with, but unfortunately that isn’t an option. I had prepared myself for some sort of immediate life or death struggle, thinking I had a form of cancer. When that didn’t happen – at least not in any obvious way – I started to let my guard down. That’s where the little things become even more dangerous. If I don’t take all of my prescriptions when I’m supposed to, or properly care for my PICC line, or keep visiting the Cancer Center 2 or 3 times a week for what has become my normal blood work/doctor visits – I could very well lose this battle. So for me, it is a struggle to remain focused. Especially considering I’m back at work now and most people I know there have moved on. I don't really look sick, and if I'm back at work then I must be cured, right? I am better than I was before I began treatment, but I can’t lose sight of the fact that I still have a long way to go. I can't let myself forget how serious this is.
I’ve also learned how much I value my family and friends. I thought I knew that before, but it’s different now. If I didn’t have the girlfriend, parents, brother, aunts & uncles, cousins, friends, boss, or co-workers that I do have, I’d be in a much worse place right now. Even my landlord sent me a get well card. I barely know my landlord. I can’t imagine dealing with this alone, and it hurts me to think that there are people out there who are forced to go it alone all the time.
I have stopped taking the Zyrtec, which was prescribed to abate possible reactions to the steroid and other medications. I’m also attempting to stop taking the Prilosec, which was for stomach/GI discomfort due to the Cyclosporine.
I am still taking the Cyclosporine, twice a day at a dosage level only recently pinpointed - after several trials at both higher and lower dosages. There is a specific level that my doctor would like to see in my blood – and for a few weeks we seemed to not be able to hit that target. I would take one dose and end up with nearly toxic levels in my blood, so then we’d drop that dose down and end up with levels that barely registered. Anyway, we eventually got it right – and I’m attempting to do it without the accompanying Prilosec (but not without the accompanying Nystatin). So far so good.
One thing I’ve learned about this whole process that I wasn’t prepared for is that it isn’t one furious sprinting battle that I’m fighting, but several much smaller long-term ones. And for me, that is harder. I’d rather attack like crazy and get it over with, but unfortunately that isn’t an option. I had prepared myself for some sort of immediate life or death struggle, thinking I had a form of cancer. When that didn’t happen – at least not in any obvious way – I started to let my guard down. That’s where the little things become even more dangerous. If I don’t take all of my prescriptions when I’m supposed to, or properly care for my PICC line, or keep visiting the Cancer Center 2 or 3 times a week for what has become my normal blood work/doctor visits – I could very well lose this battle. So for me, it is a struggle to remain focused. Especially considering I’m back at work now and most people I know there have moved on. I don't really look sick, and if I'm back at work then I must be cured, right? I am better than I was before I began treatment, but I can’t lose sight of the fact that I still have a long way to go. I can't let myself forget how serious this is.
I’ve also learned how much I value my family and friends. I thought I knew that before, but it’s different now. If I didn’t have the girlfriend, parents, brother, aunts & uncles, cousins, friends, boss, or co-workers that I do have, I’d be in a much worse place right now. Even my landlord sent me a get well card. I barely know my landlord. I can’t imagine dealing with this alone, and it hurts me to think that there are people out there who are forced to go it alone all the time.
9.26.2005
For a few weeks, my gums were very tender and I had a pretty bad canker sore. The gums would bleed whenever I tried to brush, and the sore made eating, and sometimes even talking, pretty painful. I was prescribed something called “Magic Mouthwash” – a 5 or 6 ingredient concoction that included, among other things, Benadryl, Mylanta, and liquid lidocaine. I used this mouthwash in with my prescription mouthwash Nystatin, an over the counter alcohol-free mouthwash called Prevention, and a home-made saltwater solution.
I understand that the sores are normal for somebody with AA, and not an indication that my condition might be worsening. In any case, it's all pretty much cleared up for now. The gums are still a bit tender, but that’s the worst of it. I continue to use the Nystatin and Prevention, and the other solutions will remain in my medicine cabinet until they might be needed again. Hopefully that's never.
I understand that the sores are normal for somebody with AA, and not an indication that my condition might be worsening. In any case, it's all pretty much cleared up for now. The gums are still a bit tender, but that’s the worst of it. I continue to use the Nystatin and Prevention, and the other solutions will remain in my medicine cabinet until they might be needed again. Hopefully that's never.
10.4.2005
Today I went to Saint Luke's Hospital, a place I hope to never visit again.
Don't get me wrong, the staff was super nice. All the other patients seemed a lot older than me, though. I felt very young, and very under dressed. And the whole place felt like some weird 90's country club hospital. But then again maybe I just felt uncomfortable because of the procedure I was there for.
Because the chemotherapy could possible sterilize me, I decided to have my sperm frozen. Sample collection was done at the hospital, in a very locked room within the pediatric surgery wing, at 6 am. Talk about feeling like a creeper. Not how I was used to spending my Wednesday mornings, for sure.
Don't get me wrong, the staff was super nice. All the other patients seemed a lot older than me, though. I felt very young, and very under dressed. And the whole place felt like some weird 90's country club hospital. But then again maybe I just felt uncomfortable because of the procedure I was there for.
Because the chemotherapy could possible sterilize me, I decided to have my sperm frozen. Sample collection was done at the hospital, in a very locked room within the pediatric surgery wing, at 6 am. Talk about feeling like a creeper. Not how I was used to spending my Wednesday mornings, for sure.
10.7.2005
My counts have started coming up.
Up to this point, the pattern was that I would return a low complete blood count (CBC), get a transfusion (of either platelets or whole blood), the counts would respond to that and rise a bit, and then slowly drop to start the process over again. The hope was that the time between transfusions will gradually get longer and longer, until that wonderful day that I can pull the IV out completely.
Anyway, my platelets have been hovering around the low to mid-twenties, and my hemoglobin had been hovering around the high 8 to low 9 range before they would drop and I received another transfusion. This time was different. I went in for a CBC, fully expecting to get something transfused since it had been a couple of weeks since my last blood product. But that didn’t happen. My platelets came back above thirty, and my hemoglobin came back above 10 – both firsts for me since the treatment had started. Now these numbers themselves are nothing to get excited about, since a normal range for platelets is 140-350, and normal hemoglobin is 13.6-16.5. So I’m still well below where I should be. But this was the first time that my numbers had risen without a transfusion. That means something is working, even if just a little. And that is good news.
Up to this point, the pattern was that I would return a low complete blood count (CBC), get a transfusion (of either platelets or whole blood), the counts would respond to that and rise a bit, and then slowly drop to start the process over again. The hope was that the time between transfusions will gradually get longer and longer, until that wonderful day that I can pull the IV out completely.
Anyway, my platelets have been hovering around the low to mid-twenties, and my hemoglobin had been hovering around the high 8 to low 9 range before they would drop and I received another transfusion. This time was different. I went in for a CBC, fully expecting to get something transfused since it had been a couple of weeks since my last blood product. But that didn’t happen. My platelets came back above thirty, and my hemoglobin came back above 10 – both firsts for me since the treatment had started. Now these numbers themselves are nothing to get excited about, since a normal range for platelets is 140-350, and normal hemoglobin is 13.6-16.5. So I’m still well below where I should be. But this was the first time that my numbers had risen without a transfusion. That means something is working, even if just a little. And that is good news.
10.16.2005
On Friday I visited the Siteman Cancer Center at Barnes for the first time. Despite the minor surge in my counts – preparation for a stem cell transplant still had to proceed. We don’t yet know if I will ultimately need one, but if we wait to start the process, it might end up being too late.
First I attempted to get my blood drawn at the lab, but it did not open on time and the nurses decided to send me to the doctor first so that I didn’t throw his schedule off for the day (I was his first appointment). So I headed into the office of Dr. DiPersio, the Chief of Siteman’s Oncology Division and the Director of the Bone Marrow Transplantation & Leukemia Section. Quite a mouthful.
I had looked up his resume ahead of time, and his mile long credentials list was reassurance that he was the right guy to do my transplant. I didn’t get to see him right away though; a Fellow named Dr. Kuperman came in first to run over my medical history. He seemed like a nice guy – but he was super nervous and didn't at all seem confident in what he was doing. My parents smelled this fear and just about ate him alive with their questions, most of which he couldn’t or wouldn’t answer. Luckily for him, his time with us was very short.
After he left, Dr. DiPersio came in with two medical students in tow. I don’t know if they always followed him around, or if I was of particular interest because of how rare Aplastic Anemia is. Dr. DiPersio was very personable, and did a good job of explaining the process, my condition, and what he knew or didn’t know. He also did a good job listening to and carefully answering questions that myself or my family lobbed at him. I found out that the process of setting up and finding a donor would likely take 4-6 months, and that I would probably continue my cyclosporine regimen for the next five years. As a white male, transplant history would suggest that I had an 80% chance of finding a good donor. I learned that I was a prime candidate for contracting something called Paroxysmal nocturnal hemoglobinuria (PNH), if I did not have it already. This is a condition in which a specific protein on the surface of my red blood cells would target them for premature destruction. In and of itself this is not fatal or particularly crippling – but it could lead to very dangerous blood clots later on, so it was something that I needed to be tested for about every six months.
I also learned that Dr. DiPersio had arranged for me to have bone marrow biopsy done shortly after I finished meeting with him – something I definitely would have liked to have known in advance. At the very least, I would have opted for athletic shorts and a t-shirt - not the jeans and a white dress shirt I was wearing.
After meeting with Dr. DiPersio, I met with my transplant coordinator. She gave me some more informational material, and explained her role as my primary contact at Barnes for just about anything I would need or need to know throughout the process. She then went into detail about the donor location process, something that I didn’t realize would be as complicated as it is. More than just running my info through a database, the search is quite the long and drawn out ordeal.
Then I left that set of offices and went across the hall to have my blood drawn. The lab at Barnes had never seen me before, so they didn’t realize I had a PICC line and ended up drawing from my left arm instead. That was kind of annoying. It’s not like I'm not used to getting stuck by now, but with how much hassle I go through to maintain that PICC line in my arm it better get used whenever possible.
While getting my blood drawn, I noticed that there was a doctor standing off to the side and observing me and the nurses that were hovering over me. She started to ask me questions about how I was doing, and about my medical history. She then introduced herself as Dr. Bessler, another specialist to whom I was being referred. She was an expert in the area of PNH, so my case was of interest to her. Not only as far as treating me was concerned, but also to have me participate in a study she was conducting. When my blood draw was finished, we grabbed the family members from the waiting area and went back into another office to talk about her study. Similar to Dr. DiPersio, she really seemed to know her stuff. There wasn't a question we threw at her that she wasn't able to immediately and confidently answer. Her Swiss accent didn't hurt, either. People with European accents automatically sound smarter, right?
Finally it was time for my bone marrow aspiration and skin biopsy. I was not looking forward to this. Barbara, the nurse who performed the procedure, was very forthcoming with details of what she was doing, when she was doing it, etc. This was very helpful, considering I was awake but couldn't see what was going on from my prone position. The bone marrow aspiration involves taking a toothpick sized core of bone from my iliac crest (pelvis) to be analyzed, then inserting a syringe into my bone and drawing out a sample of marrow blood. The skin biopsy (along with an oral swab) was done to get a baseline DNA for the study I was to participate in. When these were all done, Barbara patched me up with a few stitches and two band-aids. One band-aid was sparkle colored and one was traditional brown, so that I could more easily distinguish between the two sites and provide the proper "post-op" care to them.
First I attempted to get my blood drawn at the lab, but it did not open on time and the nurses decided to send me to the doctor first so that I didn’t throw his schedule off for the day (I was his first appointment). So I headed into the office of Dr. DiPersio, the Chief of Siteman’s Oncology Division and the Director of the Bone Marrow Transplantation & Leukemia Section. Quite a mouthful.
I had looked up his resume ahead of time, and his mile long credentials list was reassurance that he was the right guy to do my transplant. I didn’t get to see him right away though; a Fellow named Dr. Kuperman came in first to run over my medical history. He seemed like a nice guy – but he was super nervous and didn't at all seem confident in what he was doing. My parents smelled this fear and just about ate him alive with their questions, most of which he couldn’t or wouldn’t answer. Luckily for him, his time with us was very short.
After he left, Dr. DiPersio came in with two medical students in tow. I don’t know if they always followed him around, or if I was of particular interest because of how rare Aplastic Anemia is. Dr. DiPersio was very personable, and did a good job of explaining the process, my condition, and what he knew or didn’t know. He also did a good job listening to and carefully answering questions that myself or my family lobbed at him. I found out that the process of setting up and finding a donor would likely take 4-6 months, and that I would probably continue my cyclosporine regimen for the next five years. As a white male, transplant history would suggest that I had an 80% chance of finding a good donor. I learned that I was a prime candidate for contracting something called Paroxysmal nocturnal hemoglobinuria (PNH), if I did not have it already. This is a condition in which a specific protein on the surface of my red blood cells would target them for premature destruction. In and of itself this is not fatal or particularly crippling – but it could lead to very dangerous blood clots later on, so it was something that I needed to be tested for about every six months.
I also learned that Dr. DiPersio had arranged for me to have bone marrow biopsy done shortly after I finished meeting with him – something I definitely would have liked to have known in advance. At the very least, I would have opted for athletic shorts and a t-shirt - not the jeans and a white dress shirt I was wearing.
After meeting with Dr. DiPersio, I met with my transplant coordinator. She gave me some more informational material, and explained her role as my primary contact at Barnes for just about anything I would need or need to know throughout the process. She then went into detail about the donor location process, something that I didn’t realize would be as complicated as it is. More than just running my info through a database, the search is quite the long and drawn out ordeal.
Then I left that set of offices and went across the hall to have my blood drawn. The lab at Barnes had never seen me before, so they didn’t realize I had a PICC line and ended up drawing from my left arm instead. That was kind of annoying. It’s not like I'm not used to getting stuck by now, but with how much hassle I go through to maintain that PICC line in my arm it better get used whenever possible.
While getting my blood drawn, I noticed that there was a doctor standing off to the side and observing me and the nurses that were hovering over me. She started to ask me questions about how I was doing, and about my medical history. She then introduced herself as Dr. Bessler, another specialist to whom I was being referred. She was an expert in the area of PNH, so my case was of interest to her. Not only as far as treating me was concerned, but also to have me participate in a study she was conducting. When my blood draw was finished, we grabbed the family members from the waiting area and went back into another office to talk about her study. Similar to Dr. DiPersio, she really seemed to know her stuff. There wasn't a question we threw at her that she wasn't able to immediately and confidently answer. Her Swiss accent didn't hurt, either. People with European accents automatically sound smarter, right?
Finally it was time for my bone marrow aspiration and skin biopsy. I was not looking forward to this. Barbara, the nurse who performed the procedure, was very forthcoming with details of what she was doing, when she was doing it, etc. This was very helpful, considering I was awake but couldn't see what was going on from my prone position. The bone marrow aspiration involves taking a toothpick sized core of bone from my iliac crest (pelvis) to be analyzed, then inserting a syringe into my bone and drawing out a sample of marrow blood. The skin biopsy (along with an oral swab) was done to get a baseline DNA for the study I was to participate in. When these were all done, Barbara patched me up with a few stitches and two band-aids. One band-aid was sparkle colored and one was traditional brown, so that I could more easily distinguish between the two sites and provide the proper "post-op" care to them.
12.2.2005
My PICC line is out!
I went to Dr. Klix today, and towards the end of my visit I asked her what kind of timeline I could expect for removing my PICC. I said that I knew I couldn't get it out yet, as I will still getting blood work done every week or so. She told me that it was really more for getting whole blood or platelet transfusions - and when was the last time I had a transfusion? A quick chart lookup confirmed that it was about three months prior. She asked me, want to get it out now? Of course I immediately agreed, and about 10 minutes later one of her nurses pulled it right out of my arm.
The only (minor) downside to this is that I now have to get stuck every time they draw blood - but to me that is a small price to pay for the freedom to shower with both arms, the ability to workout, and simply not having a plastic tube and three inch square sticker coming out of my forearm. If I go back into the hospital for a transplant, I would need to get another line put in. But the procedure to put one in is something I can deal with, especially considering that the transplant is something I'm still hoping that I won't have to go through.
I went to Dr. Klix today, and towards the end of my visit I asked her what kind of timeline I could expect for removing my PICC. I said that I knew I couldn't get it out yet, as I will still getting blood work done every week or so. She told me that it was really more for getting whole blood or platelet transfusions - and when was the last time I had a transfusion? A quick chart lookup confirmed that it was about three months prior. She asked me, want to get it out now? Of course I immediately agreed, and about 10 minutes later one of her nurses pulled it right out of my arm.
The only (minor) downside to this is that I now have to get stuck every time they draw blood - but to me that is a small price to pay for the freedom to shower with both arms, the ability to workout, and simply not having a plastic tube and three inch square sticker coming out of my forearm. If I go back into the hospital for a transplant, I would need to get another line put in. But the procedure to put one in is something I can deal with, especially considering that the transplant is something I'm still hoping that I won't have to go through.
3.19.2006
I'm doing much better. Perhaps not quite out of the woods yet; but each day now is one step farther away from needing a stem cell transplant. My white blood cells and red blood cells are both pretty much normal. Platelets are low - only just over a third of what is considered normal, but still 20 times higher than when I was first admitted in July 2005. So I can't complain about that.
I see my primary hematologist/oncologist only every other month now. It was every two weeks after I had the PICC removed in December 2005. Then every three weeks. Then once a month. Now I'm getting a blood draw every month and seeing her every other. The secondary oncologist (who would be primary for transplant) only sees me every few months as well.
One thing that has not changed is my cyclosporine dose. That has remained constant for the last several months, with a dose of 350 mg/day (roughly 4.25 mg/kg). This gets me into a trough level range of 200-300, which is what Dr. Klix is shooting for. I forget a dose every now and then, but for the most part I make a small handful of pills part of my breakfast every morning and nightcap every night. I expect to keep this dose for several more months, at which point (when my numbers are considered high/stable enough) I will taper off of the drug. The hope is that the numbers will stay up after I stop the cyclosporine.
In my last visit to Dr. Klix I was cleared to visit a dentist. The visit before that I was cleared to begin swimming again, and to shave with a straight razor. I still can't have grapefruit, because of the possible interaction with my cyclosporine. And I haven't asked if I can begin using a multivitamin again. The bottle of One-A-Day Men's collecting dust in my cabinet notwithstanding, I can do most everything I would like to do.
Despite these recent months of improving health, I know I'm not even close to being cured. I still don't know exactly what caused my sickness in the first place, so I may never know if I'm going to relapse tomorrow - or if I'll never see it again. But I do know that I am doing better right now, and for that I am grateful.
I see my primary hematologist/oncologist only every other month now. It was every two weeks after I had the PICC removed in December 2005. Then every three weeks. Then once a month. Now I'm getting a blood draw every month and seeing her every other. The secondary oncologist (who would be primary for transplant) only sees me every few months as well.
One thing that has not changed is my cyclosporine dose. That has remained constant for the last several months, with a dose of 350 mg/day (roughly 4.25 mg/kg). This gets me into a trough level range of 200-300, which is what Dr. Klix is shooting for. I forget a dose every now and then, but for the most part I make a small handful of pills part of my breakfast every morning and nightcap every night. I expect to keep this dose for several more months, at which point (when my numbers are considered high/stable enough) I will taper off of the drug. The hope is that the numbers will stay up after I stop the cyclosporine.
In my last visit to Dr. Klix I was cleared to visit a dentist. The visit before that I was cleared to begin swimming again, and to shave with a straight razor. I still can't have grapefruit, because of the possible interaction with my cyclosporine. And I haven't asked if I can begin using a multivitamin again. The bottle of One-A-Day Men's collecting dust in my cabinet notwithstanding, I can do most everything I would like to do.
Despite these recent months of improving health, I know I'm not even close to being cured. I still don't know exactly what caused my sickness in the first place, so I may never know if I'm going to relapse tomorrow - or if I'll never see it again. But I do know that I am doing better right now, and for that I am grateful.
8.27.2007
Two years ago this month I was released from my stay at St. John’s Mercy Medical Center.
I still regularly see both of my hematologists/oncologists. I see my primary every three months, and the transplant specialist every six months. I have blood work done every month to month and a half.
I still take a daily 350mg dose of cyclosporine, in the form of fourteen 25mg pills. My initial doses varied, but I’ve been on the 350/day for the better part of the last two years. That means I’ve taken well over 10,000 of the stinky little pills, the smell of which I still haven’t gotten used to. However, I will take those stinky pills any day instead of the god-awful cyclosporine liquid I took in the hospital.
Did you know that cyclosporine was discovered in 1971 and is derived from a Norwegian soil fungus?
I had a very tiny blood vessel burst in my right eye and cause a distortion (like looking through water or curved glass) in the upper right-most portion of view for that eye. This happened in Spring of 2007 and from what I’ve been told, it’s very rare for somebody my age. Specifically it was a macular edema in my subretinal neovascular membrane. Was it related to my Aplastic Anemia? I don’t know, and neither did any of my doctors. I post it here in case somebody else out there with AA is in a similar situation.
One of my doctors, the transplant specialist, thinks it will be very likely that they’ll start trying to wean me off of the cyclosporine this fall. His benchmark was the two year point, which I’ve just now hit. My counts are steady, though still low on platelets, and sufficient to try and reduce medication. The theory is that they will start to lower the dose gradually, and at the same time aggressively monitor my counts. If there is a drop, I go right back on the meds – which will hopefully still be effective. Another round of ATG/chemo or even a full transplant is what I have left if cyclosporine therapy is no longer an option, so hopefully things will go well.
Correction: I was wrong about the two year cyclosporine plan. It's a five year plan.
I still regularly see both of my hematologists/oncologists. I see my primary every three months, and the transplant specialist every six months. I have blood work done every month to month and a half.
I still take a daily 350mg dose of cyclosporine, in the form of fourteen 25mg pills. My initial doses varied, but I’ve been on the 350/day for the better part of the last two years. That means I’ve taken well over 10,000 of the stinky little pills, the smell of which I still haven’t gotten used to. However, I will take those stinky pills any day instead of the god-awful cyclosporine liquid I took in the hospital.
Did you know that cyclosporine was discovered in 1971 and is derived from a Norwegian soil fungus?
I had a very tiny blood vessel burst in my right eye and cause a distortion (like looking through water or curved glass) in the upper right-most portion of view for that eye. This happened in Spring of 2007 and from what I’ve been told, it’s very rare for somebody my age. Specifically it was a macular edema in my subretinal neovascular membrane. Was it related to my Aplastic Anemia? I don’t know, and neither did any of my doctors. I post it here in case somebody else out there with AA is in a similar situation.
One of my doctors, the transplant specialist, thinks it will be very likely that they’ll start trying to wean me off of the cyclosporine this fall. His benchmark was the two year point, which I’ve just now hit. My counts are steady, though still low on platelets, and sufficient to try and reduce medication. The theory is that they will start to lower the dose gradually, and at the same time aggressively monitor my counts. If there is a drop, I go right back on the meds – which will hopefully still be effective. Another round of ATG/chemo or even a full transplant is what I have left if cyclosporine therapy is no longer an option, so hopefully things will go well.
Correction: I was wrong about the two year cyclosporine plan. It's a five year plan.
8.16.2008
It has now been three years since I was diagnosed with aplastic anemia, and subsequently released from St. John's Mercy Medical center in St. Louis.
What has changed since last year? Not much. I still take cyclosporine, twice a day. I still have annoying side effects, like increased hair growth and decreased ability to fight infections (that I now get much more often than before I had AA).
I moved to the West Coast and I live in Oregon now. Two weeks ago I met my new hematologist/oncologist for the first time, Dr. Richard Maziarz. He's a nice guy, and our first meeting was very comforting. One of my STL doctors, Dr. DiPersio, referred me to my new doc. Apparently the BMT and Hematologic Malignancy community isn't very big, and the two are friends despite being 2500 miles apart.
The new doctor practices at Oregon Health & Sciences University, which has a beautiful campus on top of a large hill in South Portland. I'm about 2 hours away, but since I'll only see Dr. Maziarz every few months it's not such a big deal.
Are you watching the summer olympics in Beijing? There is an American swimmer named Dara Torres, and she's a big story because of her age and returning to competetive swimming after retiring three times. A sidenote to her story is that her coach, Michael Lohberg, was recently diagnosed with aplastic anemia. Not much information is available about him, but I wonder if his AA is considered (like many) to be idiopathic? I only bring him up because he obviously spends much of his time around a pool and pool chemicals, like I did for many years as a swimmer and lifeguard. I wonder if there could be a connection? That's probably as much a conspiracy theory as anything else, but I doubt anybody could prove that's not the case.
I wish him and his family the best, of course. If any others are reading this that have any sort of AA and swimming/pool connection, please contact me. My email is at the top of this page.
What has changed since last year? Not much. I still take cyclosporine, twice a day. I still have annoying side effects, like increased hair growth and decreased ability to fight infections (that I now get much more often than before I had AA).
I moved to the West Coast and I live in Oregon now. Two weeks ago I met my new hematologist/oncologist for the first time, Dr. Richard Maziarz. He's a nice guy, and our first meeting was very comforting. One of my STL doctors, Dr. DiPersio, referred me to my new doc. Apparently the BMT and Hematologic Malignancy community isn't very big, and the two are friends despite being 2500 miles apart.
The new doctor practices at Oregon Health & Sciences University, which has a beautiful campus on top of a large hill in South Portland. I'm about 2 hours away, but since I'll only see Dr. Maziarz every few months it's not such a big deal.
Are you watching the summer olympics in Beijing? There is an American swimmer named Dara Torres, and she's a big story because of her age and returning to competetive swimming after retiring three times. A sidenote to her story is that her coach, Michael Lohberg, was recently diagnosed with aplastic anemia. Not much information is available about him, but I wonder if his AA is considered (like many) to be idiopathic? I only bring him up because he obviously spends much of his time around a pool and pool chemicals, like I did for many years as a swimmer and lifeguard. I wonder if there could be a connection? That's probably as much a conspiracy theory as anything else, but I doubt anybody could prove that's not the case.
I wish him and his family the best, of course. If any others are reading this that have any sort of AA and swimming/pool connection, please contact me. My email is at the top of this page.
3.17.2010
Happy St. Patrick's Day! An update to this AA blog is long overdue...
Little has changed for me since my last post. I still have aplastic anemia, and I still take a small handful of cyclosporine pills every day (and even though I'm used to them by now, they still stink). My west coast doctor, Dr. Maziarz, referred me to yet another doctor who was much closer to where I lived. So now I am under the local care of Dr. Ben Cho. He seems like a good doc, and possibly even a fellow nerd too, if the hobbies listed in his profile are any indication. He also used to work at OHSU with Dr. Maziarz, so he is quite familiar with Aplastic Anemia.
About those stinky cyclosporine pills, I had a little incident at the pharmacy a few months ago. They switched me to a different brand of pill, one that was smaller and not at all stinky. I was very happy to start taking this new brand, until I found out a month later that the pharmacy had made a mistake and the pills weren't the right cyclosporine formulation. You can read the whole story here, on my other blog. The lesson learned for me was to never underestimate how little some medical professionals I come across will know about Aplastic Anemia, or about how I specifically am being treated. Exceptions to that rule are made for my actual doctors (Klix, DiPersio, Maziarz, Cho) and anybody else that has "Hematologist" after their name. Suffice to say, I need to always be my own strongest advocate, and stay as involved as possible in decisions affecting my own health.
In other news, I recently rebuilt my non-AA blog, and now that I'm on Wordpress I've started tagging my posts in a way that lets you search them by keyword. While that site isn't specifically dedicated to AA, I have posted a few thoughts now and then related to my condition. If you go here, you'll find a list of all of those Aplastic Anemia tagged posts. As I type this out today I've only gone back and tagged about a years worth of posts so far, but eventually I'll get through all five years of archived posts.
So what's next for me?
This summer is the 5th anniversary of my initial AA diagnosis, and the start of my treatment. That's going to be a pretty big milestone, since the doctors have said all along that 5 years is when we start to consider tapering off of the cyclosporine. I'm anxious about that taper, because while it could mean I end up off the drugs (hooray!), it could also mean a relapse (boo!). A best case scenario relapse would mean I just go back on immunosuppressive therapy (IST = ATG + cyclosporine), but a less than ideal response by my blood could mean a bone marrow transplant.
To prepare for the taper, I've been cleaning up my diet and adding more exercise into my daily routine. Really though, while that will help my energy level and possibly also my waistline, it won't likely do much to stimulate my hematocrit. So I'm going to do my best to not stress over it.
I'll post again this summer after I see Dr. Maziarz about the taper. Enjoy the spring, all.
UPDATE 4/26/2010: I noticed that "cyclosporine dose" (or some aplastic anemia variant) was a very common Google search referring visitors to my site. For the record, I take 150mg BID for a total of 300mg/day. Based on my weight, that works out to about 3.75mg/kg/day. I don't recall the date we settled on this dosage, but I've been on 300mg/day for at least a couple years now.
Little has changed for me since my last post. I still have aplastic anemia, and I still take a small handful of cyclosporine pills every day (and even though I'm used to them by now, they still stink). My west coast doctor, Dr. Maziarz, referred me to yet another doctor who was much closer to where I lived. So now I am under the local care of Dr. Ben Cho. He seems like a good doc, and possibly even a fellow nerd too, if the hobbies listed in his profile are any indication. He also used to work at OHSU with Dr. Maziarz, so he is quite familiar with Aplastic Anemia.
About those stinky cyclosporine pills, I had a little incident at the pharmacy a few months ago. They switched me to a different brand of pill, one that was smaller and not at all stinky. I was very happy to start taking this new brand, until I found out a month later that the pharmacy had made a mistake and the pills weren't the right cyclosporine formulation. You can read the whole story here, on my other blog. The lesson learned for me was to never underestimate how little some medical professionals I come across will know about Aplastic Anemia, or about how I specifically am being treated. Exceptions to that rule are made for my actual doctors (Klix, DiPersio, Maziarz, Cho) and anybody else that has "Hematologist" after their name. Suffice to say, I need to always be my own strongest advocate, and stay as involved as possible in decisions affecting my own health.
In other news, I recently rebuilt my non-AA blog, and now that I'm on Wordpress I've started tagging my posts in a way that lets you search them by keyword. While that site isn't specifically dedicated to AA, I have posted a few thoughts now and then related to my condition. If you go here, you'll find a list of all of those Aplastic Anemia tagged posts. As I type this out today I've only gone back and tagged about a years worth of posts so far, but eventually I'll get through all five years of archived posts.
So what's next for me?
This summer is the 5th anniversary of my initial AA diagnosis, and the start of my treatment. That's going to be a pretty big milestone, since the doctors have said all along that 5 years is when we start to consider tapering off of the cyclosporine. I'm anxious about that taper, because while it could mean I end up off the drugs (hooray!), it could also mean a relapse (boo!). A best case scenario relapse would mean I just go back on immunosuppressive therapy (IST = ATG + cyclosporine), but a less than ideal response by my blood could mean a bone marrow transplant.
To prepare for the taper, I've been cleaning up my diet and adding more exercise into my daily routine. Really though, while that will help my energy level and possibly also my waistline, it won't likely do much to stimulate my hematocrit. So I'm going to do my best to not stress over it.
I'll post again this summer after I see Dr. Maziarz about the taper. Enjoy the spring, all.
UPDATE 4/26/2010: I noticed that "cyclosporine dose" (or some aplastic anemia variant) was a very common Google search referring visitors to my site. For the record, I take 150mg BID for a total of 300mg/day. Based on my weight, that works out to about 3.75mg/kg/day. I don't recall the date we settled on this dosage, but I've been on 300mg/day for at least a couple years now.
4.18.2010
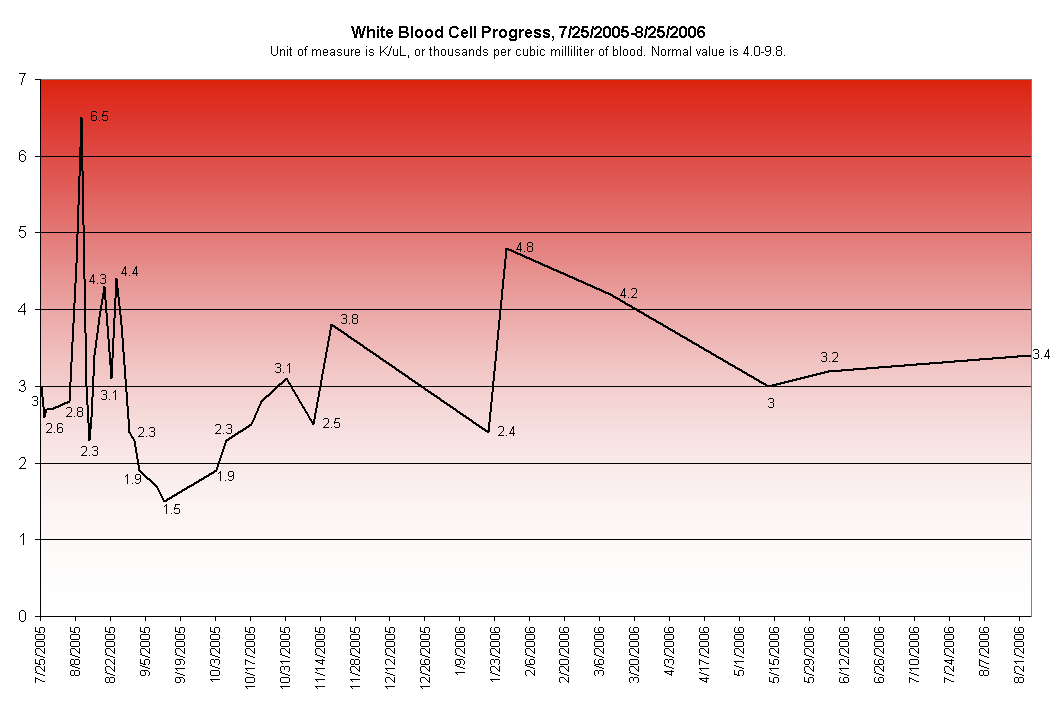
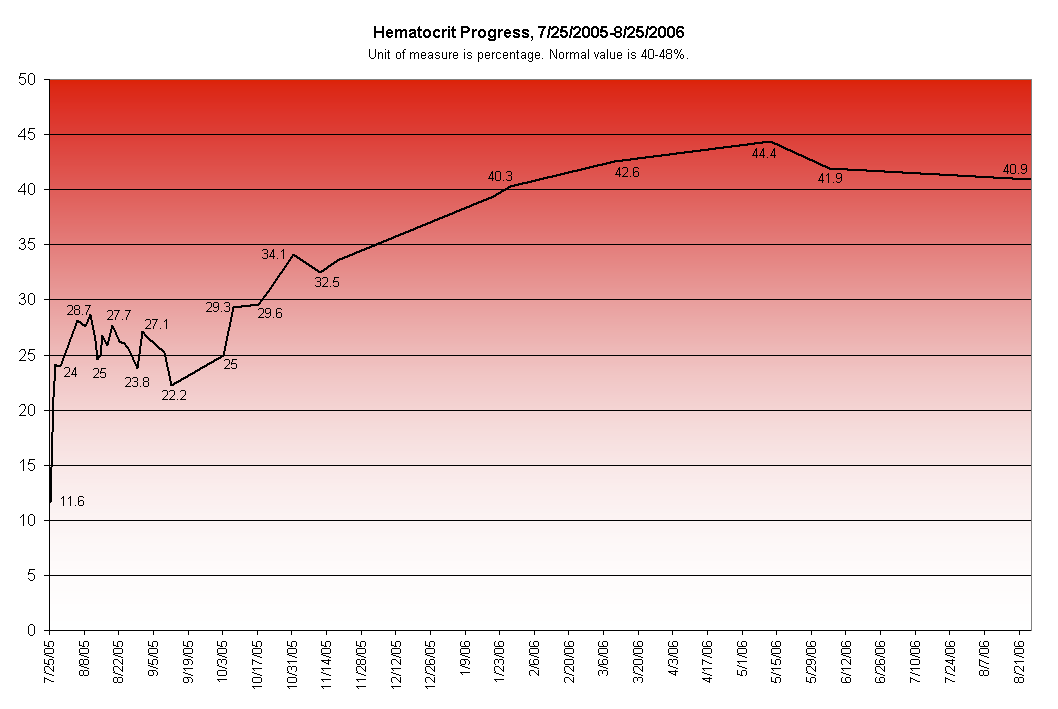
Along with the initial blood counts that I went back and added to the 8.14.2005 post, I have charted out the first 13 months of my CBC & Platelet results. At 13 months my hematocrit and hemoglobin were both up to normal ranges, and white cell was just barely under normal.
Platelet was another story; still only being about 50% of normal 13 months into treatment. This value was consistently abnormal, though, and in the 4 years since that point I have remained in the 70-80 range. So the docs theorize that this just might be what's normal for me. I can still have a high quality of life at this level, but I might need to give up the dream of becoming a knife juggler.
Platelets and Hemoglobin are on the left, and White Blood and Hematocrit are on the right. Click on any of them for a larger version.




Platelet was another story; still only being about 50% of normal 13 months into treatment. This value was consistently abnormal, though, and in the 4 years since that point I have remained in the 70-80 range. So the docs theorize that this just might be what's normal for me. I can still have a high quality of life at this level, but I might need to give up the dream of becoming a knife juggler.
Platelets and Hemoglobin are on the left, and White Blood and Hematocrit are on the right. Click on any of them for a larger version.


9.8.2010
My cyclosporine taper started this summer. For upwards of three years now, I've been taking 300mg/day, but in June I lopped off 25mg/day. July and August both also subtracted 25mg from my daily total, so this month I'm down to only 200mg/day. That monthly step down will continue until the last 75mg, at which point I'll drop 25mg every two months instead of every month. All told it's a 15 month process.
I have mixed emotions about the taper. Certainly it would be great to be off the medicine, and not pop my small handful of pills twice a day. It has side effects that I could do without, like hair growth and acne. And I wouldn't have to worry as much about elevated BP or bilirubin levels (nor would my parents). But the daily drugs have become a sort of a security blanket; something I can do, something I can control, that helps me feel slightly less powerless against Aplastic Anemia. As long as I keep taking them everything will be fine, is what I've convinced myself.
If the taper is succesful, and I'm off the cyclosporine, that doesn't mean I'm cured. In remission is probably more accurate, since I'll still need to see my doctors on a regular basis to watch for any relapses in my counts. That's my real fear, that I will eventually relapse and not be as fortunate the second time around. This time I've managed to contain the disease(s) with ATG and other chemical means. I started out as severe AA and slowly it climbed up and out to moderate AA. But what if next time I can't climb on my own to the moderate range? That means I get a BMT, the elephant in the room of anybody fighting AA.
Fortunately for me, the rational side of my brain usually starts to take over. I know that refusing to taper and just staying on the cyclosporine forever won't necessarily protect me from ever relapsing. If my counts are gonna drop again, there really isn't much I can do about it, so there isn't any point in stressing over it. And thanks to this blog I've met some great people, many of whom are BMT survivors. Their stories of survival help me know that you can beat AA, and still manage to live a long and happy life.
Note: Some of the great people I've met have their own AA blogs. I've started to list some of those blogs out in the navigation section of my site (on the left of the page, at the top) under the "Others" header. I encourage you to visit their sites and check out their stories too.
I'll see Dr. Cho next week. Since the taper started I've been getting a CBC each month, and pairing that with an actual doctor visit every other month. If I can dig up my results from the last couple CBCs, I might make another chart specific to my progress related to the taper. You can never have too many charts, right?
Also next week, I see my new primary care physician. For the last few years I've been seeing oncologists/hematologists so often that I usually just bring up non-AA issues with them, instead of seeing a general practicioner. And that's not enough, really. I need to have a separate doc who will be paying attention to the non-AA related ailments I might have. And by doctor I mean nurse practicioner, since that's who I'm signed up to see. She can apparently do almost anything the doctors can do, and when I met her the first time she didn't even bat an eye when I mentioned having Aplastic Anemia. So I'm sure she'll be great. The only problem I'll have is how to address her. Nurse Practitioner Kimball seems a bit formal. Too many syllables. But NP Kimball doesn't sound right either. Maybe just Diane?
I have mixed emotions about the taper. Certainly it would be great to be off the medicine, and not pop my small handful of pills twice a day. It has side effects that I could do without, like hair growth and acne. And I wouldn't have to worry as much about elevated BP or bilirubin levels (nor would my parents). But the daily drugs have become a sort of a security blanket; something I can do, something I can control, that helps me feel slightly less powerless against Aplastic Anemia. As long as I keep taking them everything will be fine, is what I've convinced myself.
If the taper is succesful, and I'm off the cyclosporine, that doesn't mean I'm cured. In remission is probably more accurate, since I'll still need to see my doctors on a regular basis to watch for any relapses in my counts. That's my real fear, that I will eventually relapse and not be as fortunate the second time around. This time I've managed to contain the disease(s) with ATG and other chemical means. I started out as severe AA and slowly it climbed up and out to moderate AA. But what if next time I can't climb on my own to the moderate range? That means I get a BMT, the elephant in the room of anybody fighting AA.
Fortunately for me, the rational side of my brain usually starts to take over. I know that refusing to taper and just staying on the cyclosporine forever won't necessarily protect me from ever relapsing. If my counts are gonna drop again, there really isn't much I can do about it, so there isn't any point in stressing over it. And thanks to this blog I've met some great people, many of whom are BMT survivors. Their stories of survival help me know that you can beat AA, and still manage to live a long and happy life.
Note: Some of the great people I've met have their own AA blogs. I've started to list some of those blogs out in the navigation section of my site (on the left of the page, at the top) under the "Others" header. I encourage you to visit their sites and check out their stories too.
I'll see Dr. Cho next week. Since the taper started I've been getting a CBC each month, and pairing that with an actual doctor visit every other month. If I can dig up my results from the last couple CBCs, I might make another chart specific to my progress related to the taper. You can never have too many charts, right?
Also next week, I see my new primary care physician. For the last few years I've been seeing oncologists/hematologists so often that I usually just bring up non-AA issues with them, instead of seeing a general practicioner. And that's not enough, really. I need to have a separate doc who will be paying attention to the non-AA related ailments I might have. And by doctor I mean nurse practicioner, since that's who I'm signed up to see. She can apparently do almost anything the doctors can do, and when I met her the first time she didn't even bat an eye when I mentioned having Aplastic Anemia. So I'm sure she'll be great. The only problem I'll have is how to address her. Nurse Practitioner Kimball seems a bit formal. Too many syllables. But NP Kimball doesn't sound right either. Maybe just Diane?
1.12.2011
I broke 100! For the first time in probably five years or more, I have a platelet count exceeding 100 K/ul. And while I recognize that my mark of 109 is still only about 83% of the low end of the "normal" range, it's still quite good for me. I had been happy with the 70-90 range I'd been seeing for the last few years, and just assumed that would be what was normal for me.

A friendly phlebotomist named Katie had the dubious honor ofstabbing me drawing my blood, and Dr. Cho delivered the good news. It was a very nice surprise; a good way to perk up what had been an otherwise challenging week.

Click for a larger image.
A friendly phlebotomist named Katie had the dubious honor of
4.7.2011
And... we're back. I had blood work done today, and my platelets have returned to their previous sub-100 levels. They're at 55, to be exact, significantly lower than the 70-90 range I had been seeing for the last few years. The most likely cause for the sharp drop is my cyclosporine taper. I had been on 75mg/day this month in the form of three 25mg softgels (before I started tapering last year, I was taking twelve 25mg softgels per day). In light of the platelet tumble, Dr. DiPersio bumped me back up to 100mg/day. I'll stay there until further notice, putting my taper on hold. I can't say I'm too surprised. I was expecting to have some drops before we got through the whole taper. Hopefully it's something I can pull back up without another hospital stay.
My full CBC:

Speaking of Dr. DiPersio, I moved cross-country again.
In January we packed up our things, said goodbye to the great state of Oregon, and moved into a house in Saint Louis, Missouri. The first phone calls I made were to the STL oncologists I had been seeing when I lived in Saint Louis the first time, and both doctors had room to take me on again. Dr. Mary Klix of Comprehensive Cancer Care is now my primary oncologist, and I'm also seeing Dr. John DiPersio (and Dr. Meagan Jacoby) of Siteman Cancer Center. The reason behind seeing multiple doctors is that Dr. Klix is not a transplanter, and were I to need a BMT it would be performed by Dr. DiPersio and his team.
In other news, I started a Twitter account for this blog. You can follow me via @Aplastica. I don't know that I'll be tweeting too frequently, but I will tweet a link to every new blog post I put up. So it will be another way to subscribe to the blog, if RSS isn't your thing.
My full CBC:

Click for a larger image.
Speaking of Dr. DiPersio, I moved cross-country again.
In January we packed up our things, said goodbye to the great state of Oregon, and moved into a house in Saint Louis, Missouri. The first phone calls I made were to the STL oncologists I had been seeing when I lived in Saint Louis the first time, and both doctors had room to take me on again. Dr. Mary Klix of Comprehensive Cancer Care is now my primary oncologist, and I'm also seeing Dr. John DiPersio (and Dr. Meagan Jacoby) of Siteman Cancer Center. The reason behind seeing multiple doctors is that Dr. Klix is not a transplanter, and were I to need a BMT it would be performed by Dr. DiPersio and his team.
In other news, I started a Twitter account for this blog. You can follow me via @Aplastica. I don't know that I'll be tweeting too frequently, but I will tweet a link to every new blog post I put up. So it will be another way to subscribe to the blog, if RSS isn't your thing.
8.03.2011
Dr. DiPersio and Dr. Klix both thought it wise to bump my cyclosporine up even more, so now I'm back to 300mg/day (200mg in morning and 100mg at night). I've also switched to 100mg softgels, also known as "horse pill" size. I'm so used to swallowing pills by now that the size doesn't bother me, and it is nice to have to take fewer pills.
My latest CBC results:

My reds are down just slightly, but the real news is that my platelets are back up to the high 60s, much closer to that 70-90 range I was in for so long. Seems like the increase in CyA dosage is working.
My latest CBC results:

Click for a larger image.
My reds are down just slightly, but the real news is that my platelets are back up to the high 60s, much closer to that 70-90 range I was in for so long. Seems like the increase in CyA dosage is working.
11.21.2011

Click for a larger image.
The horse pills are gone! My pharmacy seems to keep running out of my drug, and this past go around they offered me a different brand - Apotex. Compared to the same strength 100mg cap, the Apotex is considerably smaller than the Sandimmune. I asked the pharmacist twice to confirm that Apotex was legit, and not some other Cyclosporine formulation incompatible with my prescription, and it seems to be all good. These pills are easier to take, so I'll happily keep taking them until I'm forced to change brands again.
In other news, I saw Dr. DiPersio today (along with Kelly, one of his students). My latest CBC results:

Click for a larger image.
My reds and hemoglobin are both up, as are the platelets, which is always nice. 76 K/mcL is a good place for me to be. My bilirubin is also up to 2.1, which isn't really a good thing. According to DiPersio I don't really need to worry about until we hit a level of 4 or 5, though.
5.26.2012
Happy New Year! Okay, so May is a little late for that greeting. But this is my first post of 2012, so it still works.
I have two CBC results to share:


I have two CBC results to share:

Click for a larger image.
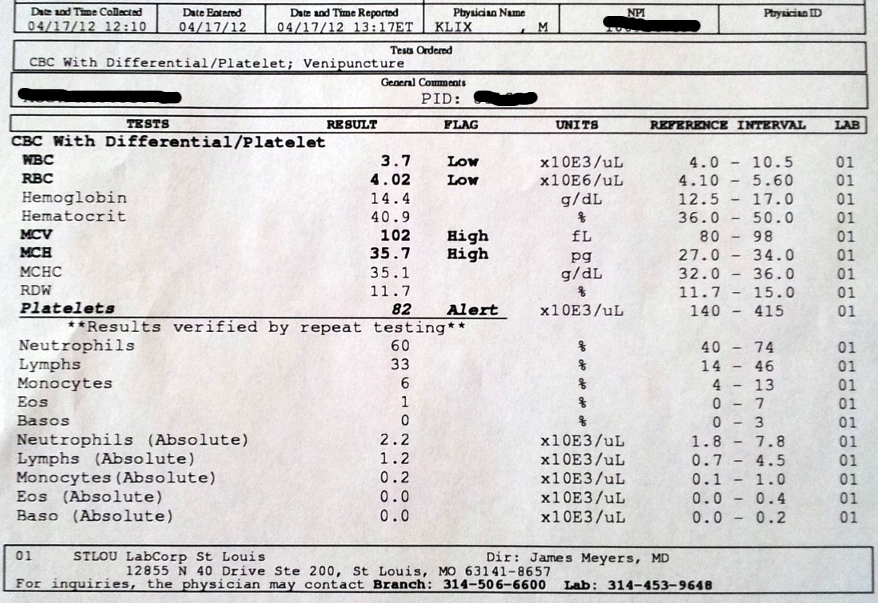
Click for a larger image.
My platelets are in the 80s both times, and that's pretty good for me. Platelets are the only thing that really fluctuate any more, and I'm happy with anything over 60.
In other news, the horse pills are back. I take 200mg/day of CyA now, with one 100mg cap in the morning and one at night.
I've also switched pharmacies, which turned out to be much more eventful than I expected. I had been with Walgreens for years. And while they had some screwups, they are on every corner so that convenience always outweighed the bad. Then my PBM, Express Scripts, got into a fight with Walgreens. Something about rates and pricing. Both sides blame the other for starting the fight, and claim that they truly only have their customers' best interests in mind. Whatever. I'll probably never know what really happened there. But what I do know is that as of January 1, 2012 my insurance was no longer welcome at Walgreens. So I was back on the market.
First, my hematologist's office set me up with the online "specialty" arm of Express Scripts. And that was a nightmare. Nobody told me what was going on, so when I tried to fill in a store it was denied because the online fill was pending. But that fill never got delivered. After multiple calls I figured out they were waiting on me... they had a wrong number for me so since that number didn't work, they just put it on hold. For two weeks, as I ran out of drugs. My doctor couldn't even figure out what was going on. So when I finally got to the bottom of it, I just had them cancel it. Considering what happened the last time I tried to use an online pharmacy run by Express Scripts, this was never really an option I seriously considered. One down.
Next, I tried Target. They probably have great customer service, right? And there is a location right down the street. Plus the bottles are cool and red, so that's a nice touch. So I logged into Target.com and applied to have my prescription transferred. Only I transferred the wrong one. It was for cyclosporine, but it was for an old quantity that was still on the list (that I hadn't filled in 6+ months). So I get an email that says my prescription will be ready Friday night. Great. I leave work and head towards the big red store, and my phone rings when I'm about 30 seconds away from parking. It's a Target Pharmacy rep, and they're calling to say they need more time to verify my prescription, on account of how long it's been since I had filled. I tell her that she must be mistaken, since I have CyA filled all the time. She's confused, and puts the actual pharmacist on the phone. He tells me, like her, that I haven't had this filled in months. I argue. Then he mentions that it's for 25mg caps, and it clicks in my head. I had been taking 100mg caps, and 25mg was the old fill. Sheepishly, I try to explain what the issue was, and that I had transferred the wrong strength. The pharmacist is not amused. In fact, he is the opposite of helpful. I tell him that I'm out of CyA, and I can't go the whole weekend without it. He tells me tough luck, and that I should page my doctor. I offer to transfer the 100mg caps over instead, and he says that since now he knows I had two different amounts, it wouldn't be ethical for him to fill either. So I tell him to forget it, and Target is off the list. Two down.
Finally, I tried CVS. They're the second biggest* pharmacy in the US behind Walgreens, and have recently expanded in the STL region, so it was a natural next step for me. And boy was I happy I found them. I transferred my prescriptions over on a Friday night, and showed up at the store on a Saturday morning to beg them for my CyA fix. They don't have it in stock, of course, but the very helpful and empathetic pharmacist tells me to stick around and he makes some calls to other nearby CVS to see what he can round up. He also has a pharmacy tech go digging around through the various Cycloporine formulations (modified vs. non-modified) and figures out that he has enough right then for a three day supply. Knowing that I am totally out, he gives me that, and arranges to have the remainder of my monthly fill delivered to his store the next day. And he does it all with a smile on his face. Can you tell that I'm a sucker for good customer service? As somebody who works in customer service, I am very intolerant of those who don't take the time to treat customers right, and very loyal to those that do. So with that, CVS takes it. I am now a happy customer of CVS store #4191 and pharmacist Adam Bradshaw. I'm a one-pharmacy kind of guy, so it's nice to be back off the market again.
*There is no source for this "Walgreens #1 followed by CVS #2" claim since I made it up based on something I think I head somewhere. It sounds good though, right?
10.23.2013
Haven't updated the blog in a while... I'm still here. I still have AA, of course, and I still gulp down cyclosporine pills day and night. Well, most nights anyway. I will admit that I occasionally fall asleep before taking my nightly dose. It's something I've been meaning to work on.
This past week I had an episode at work where I suddenly lost most vision in my left eye. It wasn't unlike when you stare into the sun, and you get those tracer things in your eye that make it hard to see for a minute? It was like that but worse, and it stuck around for about 40 minutes. I had zero peripheral vision out of that eye during that time too. I was holding up my hands on either side of my face to see if I could tell how many fingers I was holding up and on the left side I couldn't tell if the hand was even up or not. Then it went away, as quickly as it came. A few hours later my left hand started to get a little tingly, like it had fallen asleep, but that went away pretty quickly too.
The whole vision-loss experience reminded me of Summer 2005, when I lost vision in one eye before I went into the hospital for my Aplastic Anemia diagnosis. And that's a little scary. I know that my recent episode probably means that I didn't eat enough that day, and my blood counts (which tend to fluctuate) were probably on a low swing, but it's just not a good omen. I made sure to get to bed early that night, and since then I've felt fine. Luckily, I already have an appointment with my doctor coming up in just a few days, so fingers crossed that I don't have any more crazy issues before then.
This past week I had an episode at work where I suddenly lost most vision in my left eye. It wasn't unlike when you stare into the sun, and you get those tracer things in your eye that make it hard to see for a minute? It was like that but worse, and it stuck around for about 40 minutes. I had zero peripheral vision out of that eye during that time too. I was holding up my hands on either side of my face to see if I could tell how many fingers I was holding up and on the left side I couldn't tell if the hand was even up or not. Then it went away, as quickly as it came. A few hours later my left hand started to get a little tingly, like it had fallen asleep, but that went away pretty quickly too.
The whole vision-loss experience reminded me of Summer 2005, when I lost vision in one eye before I went into the hospital for my Aplastic Anemia diagnosis. And that's a little scary. I know that my recent episode probably means that I didn't eat enough that day, and my blood counts (which tend to fluctuate) were probably on a low swing, but it's just not a good omen. I made sure to get to bed early that night, and since then I've felt fine. Luckily, I already have an appointment with my doctor coming up in just a few days, so fingers crossed that I don't have any more crazy issues before then.
12.29.2013
It's not a toomah! Or in this case, it's not a stroke.
I went to go see Dr. Klix and mentioned my vision loss episode. She perked up immediately, and rattled off a list of follow-up questions. The "did you have a headache afterwards" question seemed to be a key one; I answered in the negative, though I admitted that there could have been a slight one I wasn't recalling. The symptoms I described were enough cause for concern that she referred me immediately to an imaging center where I could get an MRI of my brain. A stroke, she said, was a possibility. Her scheduler Connie found a place that would take me same day, and I drove straight there.
I had never done an MRI before, so I had no idea what I to expect.
Professional Imaging is located in the first floor of a suburban medical office building, with their entrance right off of the lobby. I stared at the building directory for a good 30 seconds before I realized that I was ten feet away from their door. The staff was friendly, and all young. Sort of like Logan's Run, an analogy that was certainly helped by the oversized, warning sign covered industrial door that seemed to take up half the wall. What went on in there? What was that throbbing womp-womp-womp noise coming from?
After filling out my patient forms I was led back to a small makeshift locker room, where I was told to leave my phone, keys, shoes, and wallet. Then I was told to sit in the hall, in a plastic chair opposite the aforementioned industrial door. I complied, but made sure to note where the nearest exit was in case I needed to make a break for it. After about 5 minutes it was my turn.
Eddie the tech opened the door and walked me into the MRI chamber. It was a barren room with a one-way window on the wall and a massive metal donut shaped machine that appeared to be sticking its tongue out at me. It was probably eight feet tall, with the "tongue" being a slim metal bed that I was directed to lay on. Eddie talked me through what was going to happen, which mostly included me staying very still and not moving. Then took my glasses and put a rubberized pair of circumaural headphones over my ears.
Eddie: What kind of music do you like?
Me: What?
Eddie: Music, for the headphones. What do you want to listen to?
Me: I dunno. Whatever.
Eddie: Rock?
Me: Yeah, that's fine.
Eddie: Pop?
Me: Sure.
Eddie: Ok.
Eddie hit a button that slowly moved my bed into the mouth of the machine, then he left the room. Or at least I assume it was a button. I was staring at the ceiling so it could have been a lever. Or a switch. I could hear music, but it was so faint that it might as well have been off. Then the machine started talking.
It started slowly, quietly, and then sped up. Womp-womp-womp. It was like a kettle drum was competing with an electrical generator. A pattern emerged. Slow fast slow repeat. It was like an all encompassing bass-heavy industrial techno. I actually liked it, and even found it to be somewhat soothing after a few minutes. I started to fall asleep towards the end, jolting awake in a hypnic jerk that left me a little freaked that my movement might have just corrupted the whole exercise. Thankfully, it hadn't. The machine stopped talking and a voice just as faint as the music came on to say something I couldn't understand.
Another tech, Joe, came into the room and pulled me out of the mouth. I was done with round one. Joe told me not to move, other than to give him my left arm. He stuck it with an IV and pumped what was probably "gado" into my veins. It was a contrast agent that was going to help make my brain veins more visible. The first round, without contrast, compared to the second round, with contrast, made it easier for the docs to tell what was going on in my grey matter. Joe finished up the IV, hit the button or lever or switch, and sent me back into the machine mouth for round two.
This time, Joe and Eddie realized how low the volume was on my headphones and cranked it up. The Steve Miller Band did their best to try and distract me from the womp-womp-womp, but I was able to tune them out and zero back in on my new kettle drum wielding friend. The second round wasn't quite as entrancing as the first though; no falling asleep this time. Pretty quickly, it seemed, Joe was back in the room again and pulling me out of the machine. He took the headphones and gave me back my glasses. Could I have a copy of the pictures, I asked? Of course, was the reply. They were already making me a disc.
I probably only spent 30 minutes in the mouth of the MRI. After they were done with me I was sent back to the locker room to gather my things, then I sat out in the waiting room for a few more minutes until Eddie came out and gave me my disc. All in all, the experience went much faster than I expected. I took my disc and went home.
That was on a Friday, so I had to wait until Monday for a nurse from Dr. Klix's office to call and tell me that I didn't have a stroke. At least it didn't look like it. They didn't know what had caused my vision loss and hand tinglin' but they were pretty sure it wasn't a stroke. That was good, somewhat anticlimactic, news.
A few weeks later the folks at Professional Imaging sent me a bill for $524, the amount I owed after adjusting for what my insurance company had covered. In fact I'm looking at the bill now, as I type this. The disc they sent me home with has now gone from "what a nice thing for them to give me" to "what an expensive little disc they could have at least bought me lunch too."
So without further ado.... my brain:


I went to go see Dr. Klix and mentioned my vision loss episode. She perked up immediately, and rattled off a list of follow-up questions. The "did you have a headache afterwards" question seemed to be a key one; I answered in the negative, though I admitted that there could have been a slight one I wasn't recalling. The symptoms I described were enough cause for concern that she referred me immediately to an imaging center where I could get an MRI of my brain. A stroke, she said, was a possibility. Her scheduler Connie found a place that would take me same day, and I drove straight there.
I had never done an MRI before, so I had no idea what I to expect.
Professional Imaging is located in the first floor of a suburban medical office building, with their entrance right off of the lobby. I stared at the building directory for a good 30 seconds before I realized that I was ten feet away from their door. The staff was friendly, and all young. Sort of like Logan's Run, an analogy that was certainly helped by the oversized, warning sign covered industrial door that seemed to take up half the wall. What went on in there? What was that throbbing womp-womp-womp noise coming from?
After filling out my patient forms I was led back to a small makeshift locker room, where I was told to leave my phone, keys, shoes, and wallet. Then I was told to sit in the hall, in a plastic chair opposite the aforementioned industrial door. I complied, but made sure to note where the nearest exit was in case I needed to make a break for it. After about 5 minutes it was my turn.
Eddie the tech opened the door and walked me into the MRI chamber. It was a barren room with a one-way window on the wall and a massive metal donut shaped machine that appeared to be sticking its tongue out at me. It was probably eight feet tall, with the "tongue" being a slim metal bed that I was directed to lay on. Eddie talked me through what was going to happen, which mostly included me staying very still and not moving. Then took my glasses and put a rubberized pair of circumaural headphones over my ears.
Eddie: What kind of music do you like?
Me: What?
Eddie: Music, for the headphones. What do you want to listen to?
Me: I dunno. Whatever.
Eddie: Rock?
Me: Yeah, that's fine.
Eddie: Pop?
Me: Sure.
Eddie: Ok.
Eddie hit a button that slowly moved my bed into the mouth of the machine, then he left the room. Or at least I assume it was a button. I was staring at the ceiling so it could have been a lever. Or a switch. I could hear music, but it was so faint that it might as well have been off. Then the machine started talking.
It started slowly, quietly, and then sped up. Womp-womp-womp. It was like a kettle drum was competing with an electrical generator. A pattern emerged. Slow fast slow repeat. It was like an all encompassing bass-heavy industrial techno. I actually liked it, and even found it to be somewhat soothing after a few minutes. I started to fall asleep towards the end, jolting awake in a hypnic jerk that left me a little freaked that my movement might have just corrupted the whole exercise. Thankfully, it hadn't. The machine stopped talking and a voice just as faint as the music came on to say something I couldn't understand.
Another tech, Joe, came into the room and pulled me out of the mouth. I was done with round one. Joe told me not to move, other than to give him my left arm. He stuck it with an IV and pumped what was probably "gado" into my veins. It was a contrast agent that was going to help make my brain veins more visible. The first round, without contrast, compared to the second round, with contrast, made it easier for the docs to tell what was going on in my grey matter. Joe finished up the IV, hit the button or lever or switch, and sent me back into the machine mouth for round two.
This time, Joe and Eddie realized how low the volume was on my headphones and cranked it up. The Steve Miller Band did their best to try and distract me from the womp-womp-womp, but I was able to tune them out and zero back in on my new kettle drum wielding friend. The second round wasn't quite as entrancing as the first though; no falling asleep this time. Pretty quickly, it seemed, Joe was back in the room again and pulling me out of the machine. He took the headphones and gave me back my glasses. Could I have a copy of the pictures, I asked? Of course, was the reply. They were already making me a disc.
I probably only spent 30 minutes in the mouth of the MRI. After they were done with me I was sent back to the locker room to gather my things, then I sat out in the waiting room for a few more minutes until Eddie came out and gave me my disc. All in all, the experience went much faster than I expected. I took my disc and went home.
That was on a Friday, so I had to wait until Monday for a nurse from Dr. Klix's office to call and tell me that I didn't have a stroke. At least it didn't look like it. They didn't know what had caused my vision loss and hand tinglin' but they were pretty sure it wasn't a stroke. That was good, somewhat anticlimactic, news.
A few weeks later the folks at Professional Imaging sent me a bill for $524, the amount I owed after adjusting for what my insurance company had covered. In fact I'm looking at the bill now, as I type this. The disc they sent me home with has now gone from "what a nice thing for them to give me" to "what an expensive little disc they could have at least bought me lunch too."
So without further ado.... my brain:

7.25.2015
It's been ten years since I was admitted to the hospital for what ended up being Aplastic Anemia. Few decisions have had a bigger impact on my life than when I made the decision to go see my doctor that day.
I get blood work done four times a year now, and I see Dr. Klix twice a year. I no longer see Dr. DiPersio, since a BMT no longer seems as likely as it once did.
I have a new job now. I left my previous employer of almost 13 years for a new opportunity at another company in town. Let me tell you, switching insurance is a real pain. All new rules, copays, websites to figure out. Not easy. I'm happy to have insurance, though. Many people in this country aren't as fortunate as I am. Medical bills from something like Aplastic Anemia can easily bankrupt a family.
Of course, I still take my daily Cyclosporine. 100Mg caps, taken twice a day. Or b.i.d. if you're into Latin. It's the same dosage I've taken for a little over three years. The smell hasn't gotten any better, but I'm pretty used to it by now.

Last year I was introduced to Gout. It's a form of arthritis where a build up of Uric Acid causes painful swelling in my toe. Like just-got-smashed-by-a-hammer kind of pain. Gout can be associated with Cyclosporine usage. It also runs in my family, so I was probably destined to get it either way.
I've come to terms with the fact that I'll likely never be cured of Aplastic Anemia. I'll be dealing with AA, Cyclosporine, and any related side-effects for the rest of my life. And that's okay. I have a good doctors and supportive friends and family to help me. We all have to go through trials in life, and if Aplastic Anemia is the worst that ever happens to me then I'll consider myself a very lucky guy.
I get blood work done four times a year now, and I see Dr. Klix twice a year. I no longer see Dr. DiPersio, since a BMT no longer seems as likely as it once did.
I have a new job now. I left my previous employer of almost 13 years for a new opportunity at another company in town. Let me tell you, switching insurance is a real pain. All new rules, copays, websites to figure out. Not easy. I'm happy to have insurance, though. Many people in this country aren't as fortunate as I am. Medical bills from something like Aplastic Anemia can easily bankrupt a family.
Of course, I still take my daily Cyclosporine. 100Mg caps, taken twice a day. Or b.i.d. if you're into Latin. It's the same dosage I've taken for a little over three years. The smell hasn't gotten any better, but I'm pretty used to it by now.

Last year I was introduced to Gout. It's a form of arthritis where a build up of Uric Acid causes painful swelling in my toe. Like just-got-smashed-by-a-hammer kind of pain. Gout can be associated with Cyclosporine usage. It also runs in my family, so I was probably destined to get it either way.
I've come to terms with the fact that I'll likely never be cured of Aplastic Anemia. I'll be dealing with AA, Cyclosporine, and any related side-effects for the rest of my life. And that's okay. I have a good doctors and supportive friends and family to help me. We all have to go through trials in life, and if Aplastic Anemia is the worst that ever happens to me then I'll consider myself a very lucky guy.
12.10.2016
Earlier this year I was forced again to switch to mail order for my prescription drugs. I held out as long as I could, but finally my insurer stopped covering my local refills so I had no choice.
The local place I had been going to is down the street, and owned by a woman who lives in my neighborhood. Great service. I will miss going there.
The local place I had been going to is down the street, and owned by a woman who lives in my neighborhood. Great service. I will miss going there.
Subscribe to:
Posts (Atom)